

- Alienshaunted : omg bro


")






- 1
- 2
umm is this shit considered an effortpost or what
The case involves a 66-year-old man who was found at home by his wife after a suicide attempt using a Franchi 12-gauge pump-action shotgun. The ammunition used was a Winchester single-round ball (commonly used for boar hunting). The man had a known history of depression and had expressed suicidal intentions prior to the event. The patient was promptly assisted and transported to the emergency department.
As evidenced by the photographic documentation taken on admission to hospital, the gunshot was fired from below, on the right side of the face, resulting in a large contused and lacerated wound with significant tissue loss and multifragmentary fractures of the facial bones . Vital signs in the emergency department showed a blood pressure of 130/75 mmHg, an oxygen saturation level (SpO2) of 94%, and a heart rate of 100 beats per minute.
A computed tomography (CT) scan of the brain, neck, facial bones, and cervical spine was performed using a multilayer spiral technique, both before and after contrast agent injection. The CT revealed a hemorrhagic contused and lacerated lesion in the right frontal region of the brain. The neck vessels did not show any significant ongoing bleeding. Facial bone reconstructions with bone window settings revealed a fracture of the right mandibular condyle, involving the mandibular angle with bone loss extending to the left hemimandible from the inferior angle to the symphysis. There were also comminuted and multifragmentary fractures involving the hard palate, ethmoid bone, orbital lamina, and left maxillary sinus. Additionally, metallic foreign bodies were observed within the right eye cavity, along with bone fragments from the orbital floor.
Given the condition of the facial bones and the evident respiratory difficulty, the patient was sedated and intubated. Fluid infusion and antibiotic prophylaxis were initiated. Considering the clinical presentation, the patient was urgently taken to the operating room to control the ongoing facial bleeding and perform a temporary tracheostomy.
A post-intubation arterial blood gas (ABG) analysis, with a fraction of inspired oxygen (FiO2) at 40%, showed the following results: pH 7.213 (normal range: 7.350–7.450), pCO2 58.3 mmHg, pO2 87.4 mmHg (normal range: 75.0–100.0 mmHg), ctHb 8.6 g/dL (normal range: 12.0–18.0 g/dL), FO2Hb 92.5% (normal range: 94.0–97.0%), and cLac 8.3 mmol/L (normal range: 0.3–2.5 mmol/L).
Five days after the initial admission, the patient's general condition stabilized and surgical reconstruction of the facial bones was carried out with three-dimensional modeled titanium reconstruction plates and meshes. Soft tissue reconstruction was achieved using local flaps. The extensive lacerated-contused wounds provided access to the damaged right mandible and orbito-malar region, which had experienced significant bone loss. Mandibular reconstruction was performed using a plate, and the orbito-maxillo-malar and nasal regions were reconstructed using appropriately modeled and fixed titanium meshes and screws. Necrotic skin flaps were excised, and skin flaps were created. Sliding flaps were used to fill the cutaneous deficits.
A postoperative CT scan was performed to confirm the presence of synthesized materials. The postoperative course was uneventful. The tracheostomy was removed 3 days after the surgery, and oral feeding was gradually reintroduced in the days that followed without oral cavity infection or functional swallowing issues. The patient was discharged from the hospital 10 days after the surgical intervention.
Follow-up visits in subsequent weeks showed regular healing and gradual stabilization of scar outcomes and functional outcomes. Six months post-surgery, despite satisfactory wound healing, the patient was offered a facial reconstruction procedure using microvascular free flaps to achieve better aesthetic and functional restoration of the face and facial skeleton. However, the patient declined the proposed intervention, expressing satisfaction with the results that had already been achieved.





- 4
- 5
I lied. I have info. a lot. IS THIS AN EFFORTPOST? IS IT??
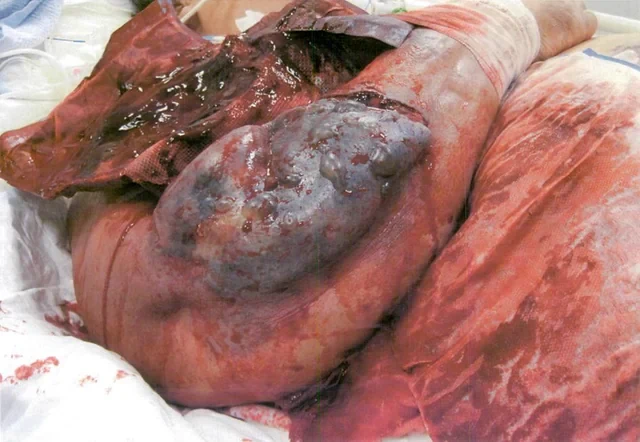
A 45 year old woman had a bariatric gastric bypass surgical operation. A few years before the operation she had a weight of 192 kg (BMI 65). Over a two years period she was able to reduce her weight to 149 kg. This preoperative weight of 149 kg was stable over the last four months before the gastric bypass operation. She had a medical history of insulin-dependent diabetes mellitus and severe psoriasis. She had also been hospitalised with erysipelas and ulcers on the lower extremities a few years prior to having gastric bypass surgery.
Though she received postoperative advice from a dietician about the importance of eating a vitamin rich diet, she continued with an insufficient diet in order to obtain further weight loss. Three months postoperatively she had lost further 20 kg in weight. At the same time she began to develop painful swelling, bruising and small ulcers on the lower extremities. She was hospitalised at the local hospital with fever one week after these symptoms appeared. Within the next 24 hours she developed purpura on the lower extremities and a sepsis like condition. Due to this she was transferred to Intensive care unit (ICU) at Odense University hospital. Within days she developed multiple organ dysfunction syndrome with cerebral, respiratory, circulatory and renal failure. It was necessary to intubate and ventilate the patient and renal failure was treated with continuous renal replacement therapy (CRRT). To restore the circulation it was necessary to treat the patient with a large amount of intravenous fluids and vasopressor agents. Infected leg ulcers were suspected to be the focus for sepsis. After appropriate samples of blood and secretion were taken for cultures, broad-spectrum antibiotic was initiated. No bacteria occurred in the cultures and the patient showed no signs of improvement on antibiotic therapy. In contrast the changes in the skin progressed with increasing erythema, and ecchymosis forming a painful, confluent purpuric plaques and bullae. Minimal trauma to the skin resulted in petechiae and confluent purpuric plaques. It was estimated that 30% of the skin was affected by confluent purpuric plaques. As a result of these haemorrhagic bullae the patient was continuously bleeding from the skin. On the worst days the blood loss from the skin was estimated to be 61 per day. In addition to blood loss the patient lost a large amount of fluid from the skin-estimated on the worst days to be 201 per day. The patient's lips were covered with haemorrhagic crust but no major gingival bleeding was observed. Skin biopsy was performed. This biopsy showed diffuse extravasation of erythrocytes but no hyperkeratosis or “corkscrew hair”. The subdermal tissue was vital. A biopsy from the bone marrow was without any sign of malignancy.
Over the three weeks in the ICU it became obvious that the skin changes and the massive loss of blood and fluid from the skin were not in accordance with a diagnosis of sepsis. It was proposed that the massive bleeding from the skin might be due to scurvy. A blood sample for the analysis of serum-ascorbic acid levels was taken and the patient was treated with enteral ascorbic acid at a dose of 2 g per day. The blood sample showed a serum-ascorbic acid concentration of 6.6 (normal range 26 - 85 μmol per l). After two days of vitamin-C treatment the patient's condition began gradually to improve. The skin changes gradually disappeared, haemodynamics improved, the patient regained her renal function and could be weaned from the ventilator. A few weeks after the start of ascorbic acid treatment the patient could be transferred to the medical ward.
my bad to all the big FAT misspells. I'm dyslexic, spare me, oh sexy one.



- 12
- 14
Active:
Inactive:
YouTube, (most) News Sites & Reddit don't count due to a majority of reasons.
Top Poster of the Day:
 TheBillCollector
TheBillCollector
Deaths Today: 0
Current Registered Users: 2,023,002
 BROWSE EFFORTPOSTS
SITE GUIDE
PING GROUPS
BROWSE EFFORTPOSTS
SITE GUIDE
PING GROUPS
 Slavshit
Slavshit

 Sandshit
Sandshit
