




.webp?x=8 "Cat Ears (wiggly) - MEOW MEOW MEOW MEOW MEOW MEOW MEOW")


- 17
- 56
Leaked photos from a Chinese morgue show the autopsy of a brutally murdered woman. Her attacker stabbed her multiple times and slit her throat. The wounds on her hands indicate that the victim was actively trying to defend herself.
No idea if the first image is a repost, but also, more photos:

















- 5
- 4
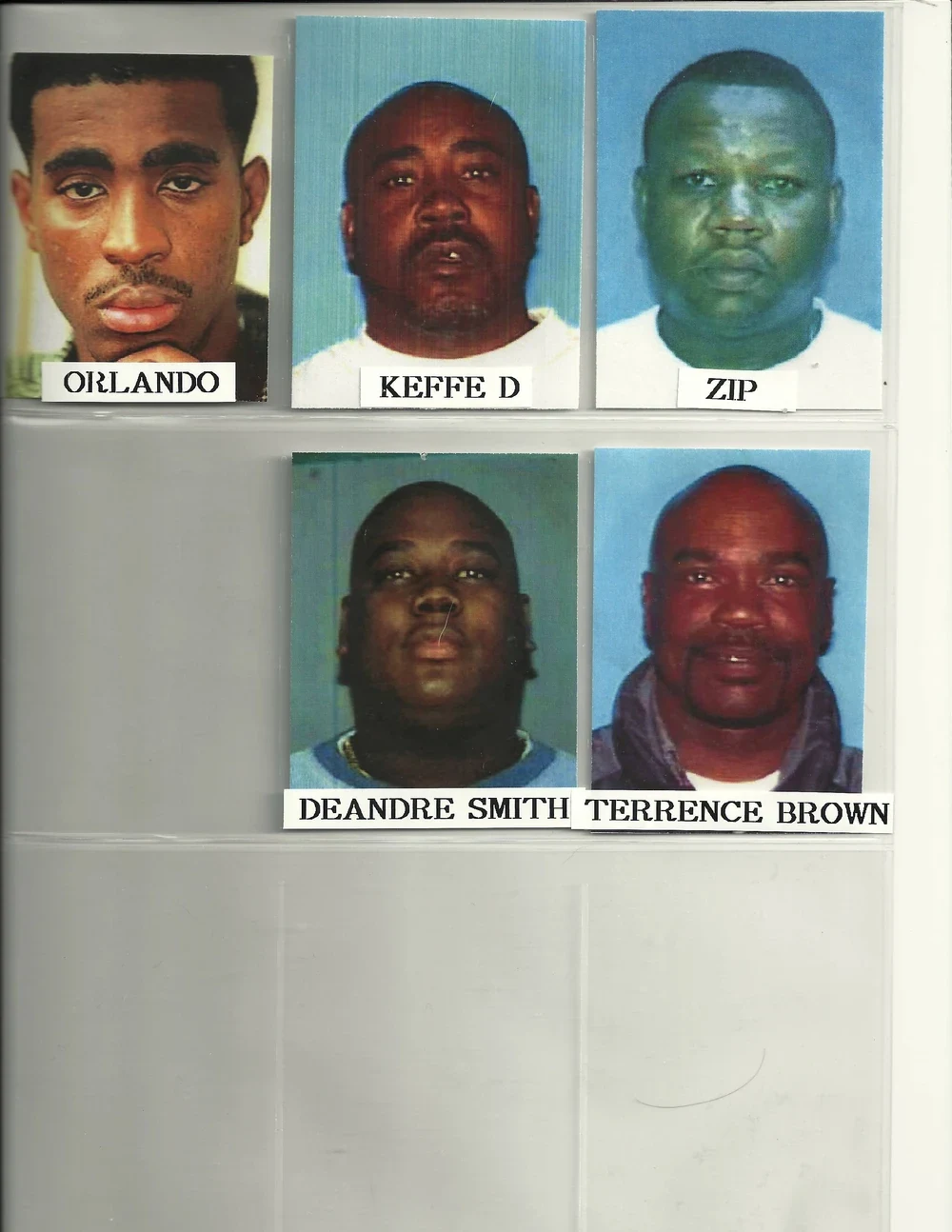
American rapper Tupac Shakur passed away on September 13, 1996, six days after sustaining multiple gunshot wounds in a drive-by shooting in Las Vegas, Nevada. The incident occurred at 11:15 pm while Shakur's car was halted at a red light on East Flamingo Road and Koval Lane. He was struck four times by gunfire from a .40-caliber Glock, sustaining injuries to his chest, arm, and thigh. Despite medical efforts, Shakur succumbed to his wounds at the University Medical Center of Southern Nevada.

Though the identity of his assailant remains elusive, speculation suggests involvement from Orlando Anderson, purportedly a member of the Crips gang. This suspicion stems from an altercation earlier in which Shakur and his associates confronted Anderson, who had allegedly clashed with them prior to the shooting. The murder case of Shakur remains unresolved officially.
Background:
See East Coast-West Coast hip hop rivalry for additional context.
On November 30, 1994, Shakur encountered a robbery and subsequent shooting at Quad Recording Studios in Manhattan, where he sustained five gunshot wounds. Accusations were directed at Sean Combs, Andre Harrell, and Christopher "The Notorious B.I.G." Wallace, present during the incident. Shakur also harbored suspicions against Randy "Stretch" Walker, accompanying him at the time.
During Shakur's incarceration for sexual assault, Wallace released the contentious track "Who Shot Ya?" interpreted by Shakur as a taunt regarding his prior assault. Shakur retaliated with numerous diss tracks targeting the East Coast hip hop scene, primarily aimed at Combs, Wallace, and Bad Boy Entertainment. This marked the onset of the coastal rivalry that characterized mid-1990s hip hop, often associated with the untimely deaths of Shakur and Wallace.
Las Vegas, Nevada:
On September 6, 1996, at 11:30 pm, Shakur left Lacy Street Production Studio in Los Angeles, concluding the filming of his music video "Toss It Up." Following a brief stop at his Calabasas mansion, he departed for Las Vegas with his cousin Jamala Lesane. Shakur attended the Mike Tyson - Bruce Sheldon boxing match at the MGM Grand, accompanied by Suge Knight, before his scheduled performance at Club 662.
Upon arrival in Las Vegas at 3 pm, Shakur left his girlfriend and cousin in their hotel room to engage in gambling at a nearby casino, accompanied by his entourage, including bodyguard Frank Alexander and members of The Outlawz. After witnessing Tyson's victory, an altercation ensued in the MGM Grand lobby between Death Row affiliates and Orlando "Baby Lane" Anderson, allegedly linked to a previous robbery involving Death Row associates. Amidst the scuffle, Shakur refrained from wearing his bulletproof vest, opting to change clothes before his performance at Club 662.
Subsequently, Shakur departed for Suge Knight's residence, where he and Knight engaged in private conversation, leading Shakur to request Alexander's presence in a separate vehicle. The Death Row entourage, comprising ten cars, departed from Knight's mansion, with Shakur and Knight occupying Knight's BMW 750.
Between 10:50 - 10:55 pm, the final photograph of Shakur was captured at a red light. Later, Knight's vehicle encountered a police stop for infractions, with no penalties issued. Around 11:15 pm, at the intersection of East Flamingo Road and Koval Lane, Knight's BMW was ambushed by gunfire from a white Cadillac, resulting in Shakur's fatal injuries and Knight sustaining a head wound.

Following the shooting, Knight maneuvered the vehicle to seek medical assistance. Despite efforts to revive Shakur, he succumbed to his injuries at the University Medical Center on September 13, 1996. The official cause of death cited respiratory failure and cardiopulmonary arrest due to multiple gunshot wounds. Shakur's remains were cremated the following day, fulfilling his request for a portion of his ashes to be mixed with marijuana and consumed by members of The Outlawz. His posthumous album, "The Don Killuminati: The 7 Day Theory," was released on November 5, 1996, by Death Row Records.
Here are the suspects :








- 25
- 19

India.
Dhanika suffers from leukemia, which caused her eyes to bulge out of her head and even bleed while the infection was occurring. She lives with her mother in poor conditions in a small village. Her mother could not afford treatment, and so the disease has reached this horrific stage.
(Idk if it's a repost or not.)


- 7
- 13
I lied. I have info. a lot. IS THIS AN EFFORTPOST? IS IT??
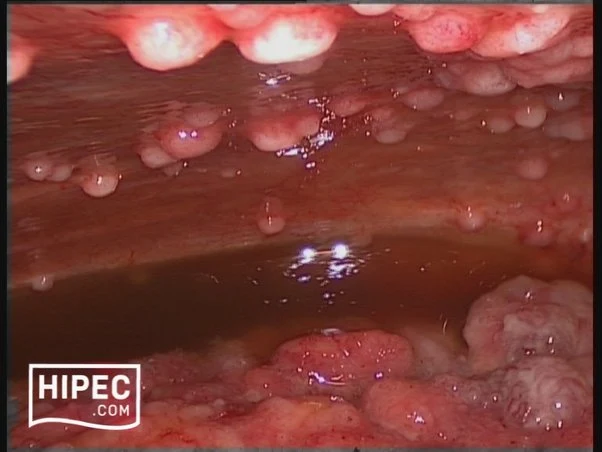
A 45 year old woman had a bariatric gastric bypass surgical operation. A few years before the operation she had a weight of 192 kg (BMI 65). Over a two years period she was able to reduce her weight to 149 kg. This preoperative weight of 149 kg was stable over the last four months before the gastric bypass operation. She had a medical history of insulin-dependent diabetes mellitus and severe psoriasis. She had also been hospitalised with erysipelas and ulcers on the lower extremities a few years prior to having gastric bypass surgery.
Though she received postoperative advice from a dietician about the importance of eating a vitamin rich diet, she continued with an insufficient diet in order to obtain further weight loss. Three months postoperatively she had lost further 20 kg in weight. At the same time she began to develop painful swelling, bruising and small ulcers on the lower extremities. She was hospitalised at the local hospital with fever one week after these symptoms appeared. Within the next 24 hours she developed purpura on the lower extremities and a sepsis like condition. Due to this she was transferred to Intensive care unit (ICU) at Odense University hospital. Within days she developed multiple organ dysfunction syndrome with cerebral, respiratory, circulatory and renal failure. It was necessary to intubate and ventilate the patient and renal failure was treated with continuous renal replacement therapy (CRRT). To restore the circulation it was necessary to treat the patient with a large amount of intravenous fluids and vasopressor agents. Infected leg ulcers were suspected to be the focus for sepsis. After appropriate samples of blood and secretion were taken for cultures, broad-spectrum antibiotic was initiated. No bacteria occurred in the cultures and the patient showed no signs of improvement on antibiotic therapy. In contrast the changes in the skin progressed with increasing erythema, and ecchymosis forming a painful, confluent purpuric plaques and bullae. Minimal trauma to the skin resulted in petechiae and confluent purpuric plaques. It was estimated that 30% of the skin was affected by confluent purpuric plaques. As a result of these haemorrhagic bullae the patient was continuously bleeding from the skin. On the worst days the blood loss from the skin was estimated to be 61 per day. In addition to blood loss the patient lost a large amount of fluid from the skin-estimated on the worst days to be 201 per day. The patient's lips were covered with haemorrhagic crust but no major gingival bleeding was observed. Skin biopsy was performed. This biopsy showed diffuse extravasation of erythrocytes but no hyperkeratosis or “corkscrew hair”. The subdermal tissue was vital. A biopsy from the bone marrow was without any sign of malignancy.
Over the three weeks in the ICU it became obvious that the skin changes and the massive loss of blood and fluid from the skin were not in accordance with a diagnosis of sepsis. It was proposed that the massive bleeding from the skin might be due to scurvy. A blood sample for the analysis of serum-ascorbic acid levels was taken and the patient was treated with enteral ascorbic acid at a dose of 2 g per day. The blood sample showed a serum-ascorbic acid concentration of 6.6 (normal range 26 - 85 μmol per l). After two days of vitamin-C treatment the patient's condition began gradually to improve. The skin changes gradually disappeared, haemodynamics improved, the patient regained her renal function and could be weaned from the ventilator. A few weeks after the start of ascorbic acid treatment the patient could be transferred to the medical ward.
my bad to all the big FAT misspells. I'm dyslexic, spare me, oh sexy one.












- 12
- 27
quite lovely! I don't have any further info tho, so don't ask! 



- 2
- 18
A_ intra-operative view showing the dartos myo cutneous flaps harvested from the lateral part of the scrotum.
B_ the dartos myo cutneous flaps are rotated to cover the anterior surface of the shaft and sutured on the midline.

 local whore
local whore 
- 13
- 31
Definition
Oxford Languages:
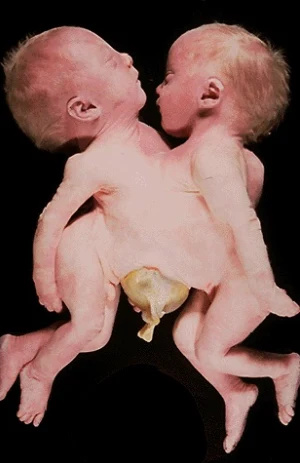
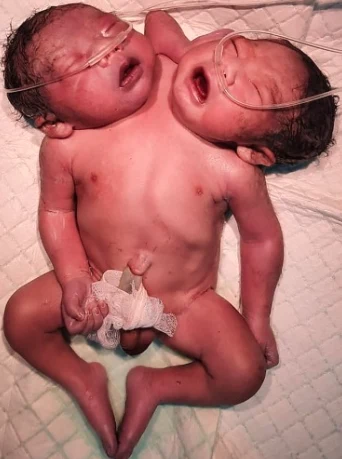
Twins that are physically joined at birth, sometimes sharing organs, and in some cases separable by surgery (depending on the degree of fusion).
Medical Definition:
Conjoined twins are two babies who are born physically connected to each other.
Causes
Conjoined twins develope when an early embryo only partially seperates to form two children. That means, two children develope but they stay physically connected. It is believed that this only occurs when an embryo of identical twins (monozygotic twins) splits later than usual, causing the seperation to stop before the process is complete. There is also a theory that the bodies fuse together after their development, however this hasn't been proven yet.
Cases of Conjoined Twins
Chest: These twins are called Thoracopagus twins. They are joined at their chest, facing each other. They may share a heart and liver.

Abdomen: Omphalopagus twins are joined near the bellybutton. They often share a liver and the upper digestive tract. Some twins share the lower part of the small intestine (ileum) and the longest part of the large intestine (colon). They never share a heart.

Base of the Spine: Pygopagus twins are commonly joined back to back at the base of the spine and the buttocks. Some pygopagus twins share the lower gastrointestinal tract, some even their genitals and urinary organs.

Length of the Spine: Rachipagus, also called rachiopagus, twins are joined back to back along the length of the spine. Often only one of the twins is fully developed. The other one is seen as a Parasitic Rachipagus Twin. This type is very rare.

Pelvis: Ischiopagus twins are joined at the pelvis, they can be face to face or end to end. They often share the gastrointestinal tract, as well as liver, genitals and urinary organs. Some even share a leg or two, but that is very rare.


Trunk: Parapagus twins are joined side to side at the pelvis and part or all of the belly (abdomen) and chest, but with separate heads. The twins can have two, three or four arms and two or three legs.
Head: Craniopagus twins are joined at the back, top or side of the head, but not the face. Craniopagus twins share a portion of the skull. But their brains are usually separate, though they may share some brain tissue.

Head and chest: Cephalopagus twins are joined at the head and upper body. The faces are on opposite sides of a single shared head, and they share a brain. These twins rarely survive.

Diagnosis
Conjoined twins are often diagnosed in the early stages of pregnancy with a prenatal ultrasound. A thorough prenatal evaluation is particularly important for conjoined twins, as the location and extent of where the twins are joined and what organs are shared plays a crucial role in deciding whether the twins will be separable. To thouroughly diagnose conjoined twins, a fetal ultrasound, a fetal echocardiogram and an Ultrafast fetal MRI are used.
Seperation Surgery
If the conjoined twins are candidates for separation surgery, CHOP's pediatric surgical team (which may include general surgeons, plastic and reconstructive surgeons, neurosurgeons and other surgical specialties) will work with a multidisciplinary team to monitor the babies and determine the timeline and approach for the surgical procedure. Specialists involved in your care will likely include neonatologists, cardiologists, advanced practice nurses and maternal-fetal medicine specialists, among others.
One of the many procedures required to prepare twins for separation is the insertion of tissue expanders to increase the skin surface available to cover exposed tissue after surgery.
As separated twins recover after surgery, they are closely followed by nutritionists, developmental pediatricians and other specialists to ensure their ability to thrive and grow.
When the conjoined twins share a heart, successful surgical division is usually not possible.
Notes: I couldn't find video material of a seperation surgery, so if you have some, it would be greatly appretiate it if I can add them to my post!

")







 Carioca fofa
Carioca fofa 



- 9
- 14
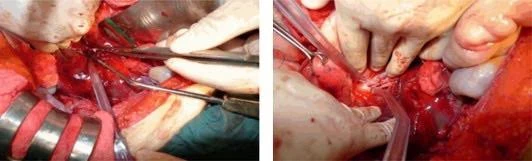
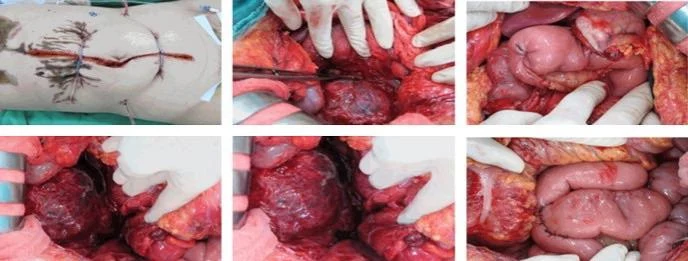
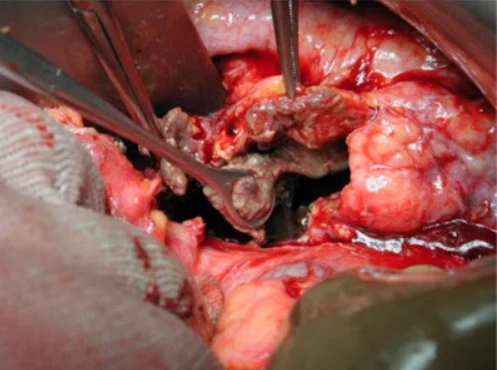
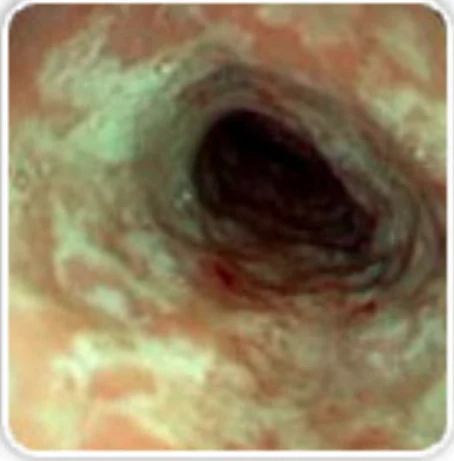
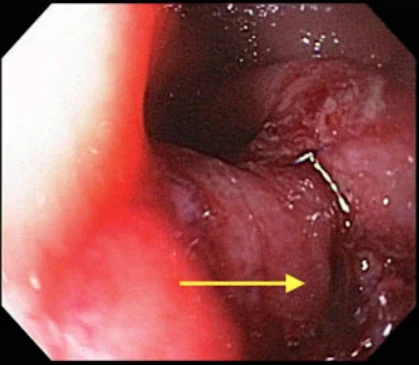
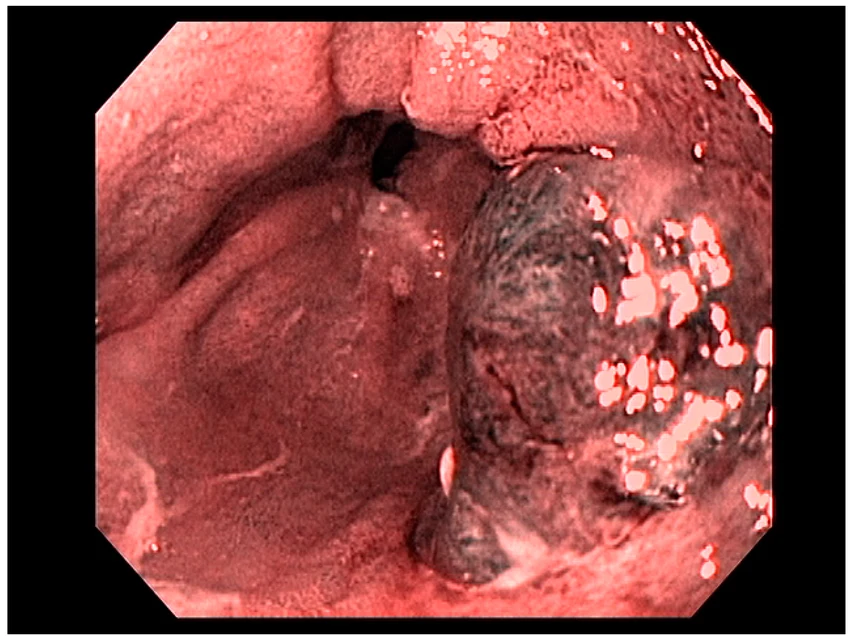
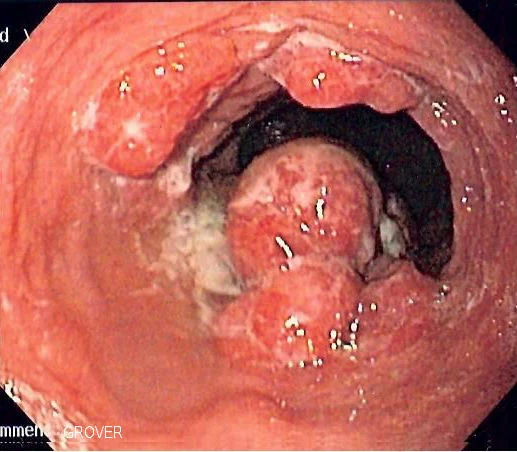
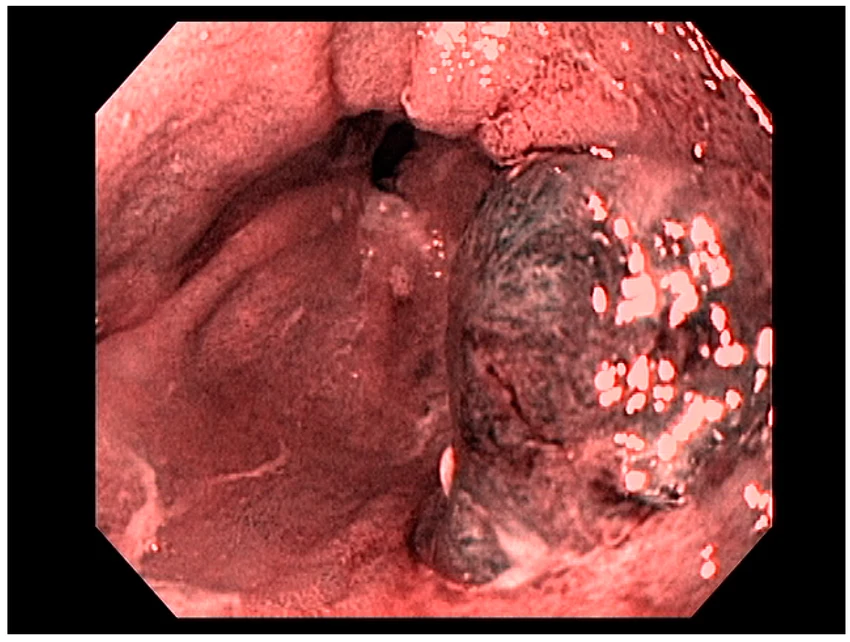
A 38-year-old woman was injured in a domestic dispute with her ex-husband. She was stabbed in her belly and splashed with sulfuric acid. Upon presentation to our emergency department, a physical examination showed one 5-cm-long, longitudinal, penetrating wound in the upper midline abdominal region, with a sharp demarcation and exposure of abdominal viscera. In addition, she exhibited second- to third-degree chemical burn injuries over her chin, anterior chest, and both upper limbs covering 15% of the total body surface area (Fig. 1). The injury severity score exceeded 16. While in the emergency department, the patient went into hypovolemic shock. Fluid resuscitation and blood transfusion were performed after a quick initial survey. Substantial saline irrigation over the burn lesions was performed. Emergency damage control surgery was commenced, under general anesthesia and using exploratory laparoscopy, to determine the extent of bleeding. Repair of the severed inferior vena cava (IVC) and a partial gastrectomy were performed. Near-total transection of the first portion of the duodenum, and a perforation of the IVC (Fig. 2) of approximately 2.5 cm were noted during the operation.
After the surgery, the patient was admitted to our intensive care unit for further treatment. Coagulopathy occurred after substantial blood transfusions because of the activation and depletion of coagulation factors secondary to tissue trauma. Empiric antibiotics with ampicillin and sulbactam were administered upon admission. In addition, we consulted a nutritional support team doctor in evaluating and managing her nutritional condition.
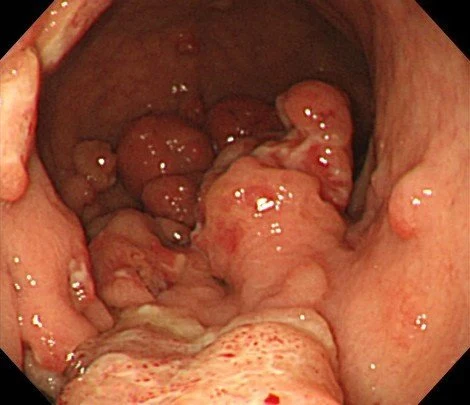
Because of the relatively stable condition of this patient, exploratory laparoscopy with a Roux-en-Y gastrojejunostomy and primary suture of the duodenum was performed as a second-stage operation (Fig. 3). In addition, we performed early debridement of the chemical burn wound on the 3rd day postinjury. Fluid resuscitation was performed according to the Parkland formula and adjusted according to the urine output. Several skin grafting procedures were performed to cover the wound. A consultation with a psychiatrist was arranged to establish and evaluate the patient's rehabilitation program.
After 1 year of follow-up, the patient had fully recovered. She had a full range of motion in her neck and both upper limbs and exhibited no scar contracture (Fig. 4).

year later :

https://www.sciencedirect.com/science/article/pii/S1682606X15000031

- 11
- 14
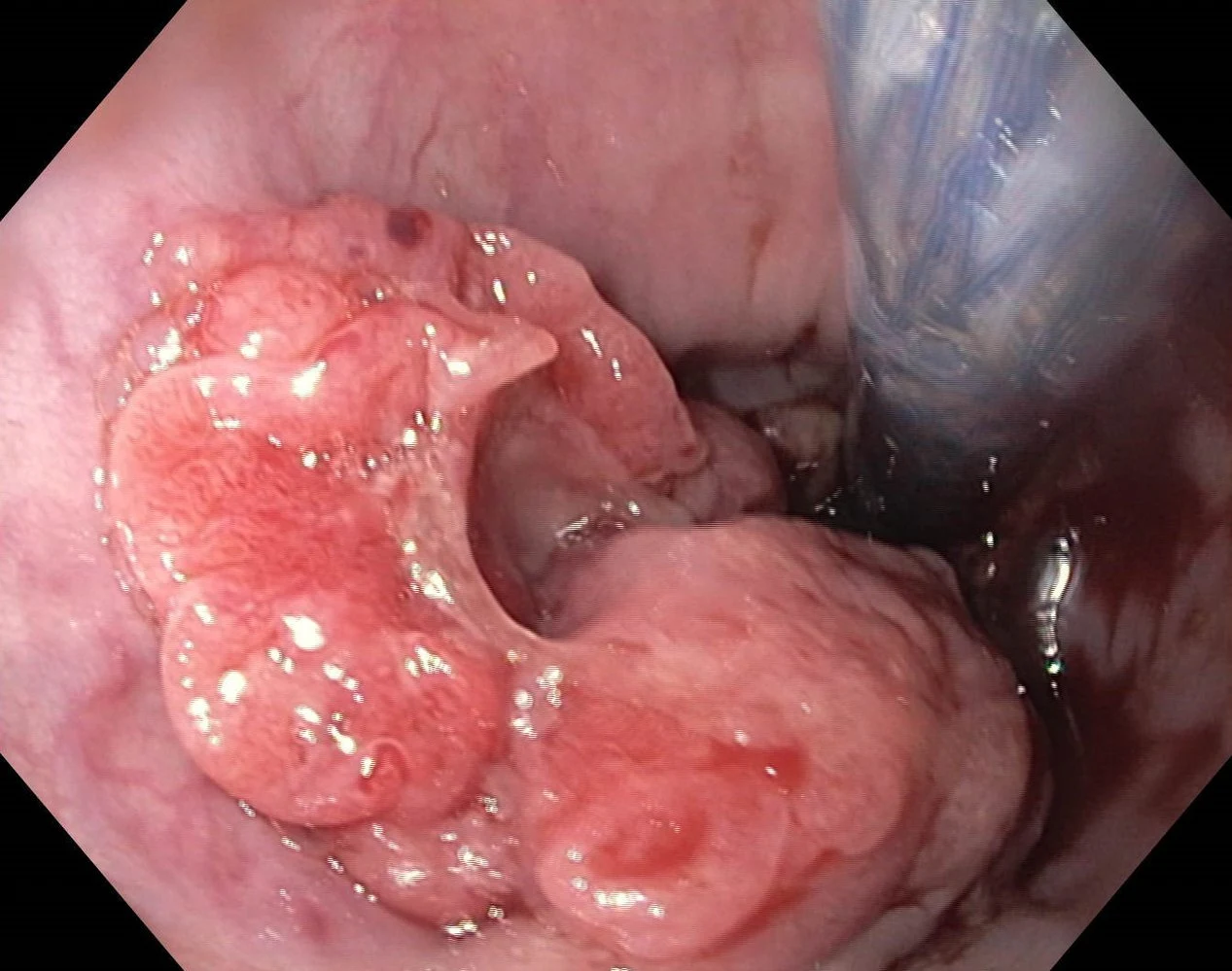
Introduction Clitoromegaly is an abnormality condition commonly related to congenital adrenal hyperplasia; it is rare due to idiopathic. Until now, there is no report about idiopathic clitoromegaly who reach adulthood and evaluation of their sexual life after reconstructive surgery. Presentation of case We presented an adult female patient with chief complain of enlarged clitoris since birth. The phenotypic appearance of ambiguous external genitalia resembling severe hypospadias with scrotal bifid. Other female secondary sexual characteristics were normal. The karyotype test result was 46 XX. We did genitalia reconstruction with nerve-sparing clitoroplasty, oral mucosal graft vaginoplasty, and labioplasty. Discussion Many factors contribute to clitoromegaly which emerge transiently during the intrauterine period. Our case was unique due to clitoromegaly persistence until adulthood and can not be explained by any hypotheses. Adult females with clitoromegaly and urogenital sinus (UGS) bring a specific problem, especially to their sexual life. The reconstructive surgery should consider the phenotype of genital anatomy, preservation of clitoral neurovascular bundles, and adequate dimension of the vagina. Oral mucosal graft is an option as substitutive materials that can be used for vaginal augmentation. Conclusion This is a case report of adult female idiopathic clitoromegaly patient. Scrutinized evaluation is needed to confirm the diagnosis. Many aspects should be considered to perform feminizing genitoplasty. The surgery did not reduce the sensitivity of clitoris and allow the patient to do sexual activity after marriage during a one-year follow up.








- 53
- 174
What is Bulima Nervosa?
Bulimia Nervosa is an eating disorder and a mental illness.
Symptoms of Bulimia Nervosa can include
eating a large amount of food (binge eating)
self-induced vomiting (purgeing)
excessive laxative use
fasting
excessive exercise
using medication inappropriatly to reduce weight
Psychological symptoms of Bulimia Nervosa can include
preoccupation or obsession with eating, dieting, exercise or body image
fear of gaining weight
sensitivity to comments about eating, dieting, exercise or body image
feelings of shame, guilt and disgust, especially after eating and/or purging
a distorted body image or extreme dissatisfaction with body shape
anxiety or irritability around meal times
low self-esteem, depression, anxiety or suicidality
Behavioural symptoms of Bulimia Nervosa can include
repetitive dieting behaviour (such as counting calories, fasting, skipping meals, avoiding certain food groups)
excessive exercise, even when sick or injured
avoiding social situations
eating alone or in secret, avoiding other people at meal times
hiding food
frequent trips to the bathroom during or after eating
use of laxatives, enemas, diuretics or appetite suppressants
spending large amounts of money on food
self-harming behaviour, substance misuse and suicidality
The effects of Bulimia Nervosa on the human body
incontinence (urinal and fecal)
gastrointestinal conditions associated with compensatory behaviours
heart-related issues
weakened bones (osteoporosis)
infertility in men and women
electrolyte imbalance from self-induced vomiting – this can cause severe dehydration, and damage nerves, muscles and organs
subconjunctival hemorrhage of the eye from the strain of purging

tooth cavities, diseased gums, and irreversible enamel erosion caused by excessive acid in the mouth from purging
[Screenshot 2024-04-26 10.2.08.png]
hemorrhoids caused by weakened rectal walls from the strain of purging

prolapsed bowel as a result of rectal walls being weakened by the strain of purging

acute pancreatitis
swollen salivary glands

peptic ulcer caused by excess acid in the stomach

gastric rupture (ruptured stomach) caused by periods of bingeing

esophagitis from purging
tear in the esophagus from purging

rupture of the esophagus
small cuts across the back of the hand due to self-induced vomiting

water retention, swelling, and abdominal bloating

inflammation of the throat from purging

death
I've made another post about the last picture specifically and their autopsy report! Feel free to look at it 
This post is supposed to show the dangers of Bulimia Nervosa and it is NOT meant to 'glorify' eating disorders!!!




- 9
- 24
Just found this video while scrolling on my old phones camera roll, I have no info whatsoever about it but I know it's self inflicted in..some way 



- 6
- 20
In Brazil, a "stone child" was found inside an 81-year-old woman who had been inside her for 56 years.
The fetus died, but the woman did not go to the doctors, and the child simply petrified there.
- 4
- 7
Definition
Obesity is a chronic complex disease defined by excessive fat deposits that can impair health.
Effects of obesity on the human body
Physical effects that can appear:
higher risk for cancer (breast, endometrial, ovarian, colorectal, esophageal, kidney, pancreatic, prostate)
type 2 diabetes
hypertension
stroke
coronary artery disease
congestive heart failure
asthma
chronic back pain
osteoarthritis
pulmonary embolism
gallstones
gallbladder disease
an increased risk of disability
high blood pressure
high cholesterol
musculoskeletal discomfort
breathing problems
'smushed' organs
fertility problems
sexual function problems
Emotional effects that can appear:
risk of low self-esteem
binge eating disorder
mood disorders
motivational disorders
impaired body image


Fat-Loss Surgeries:
- 14
- 42
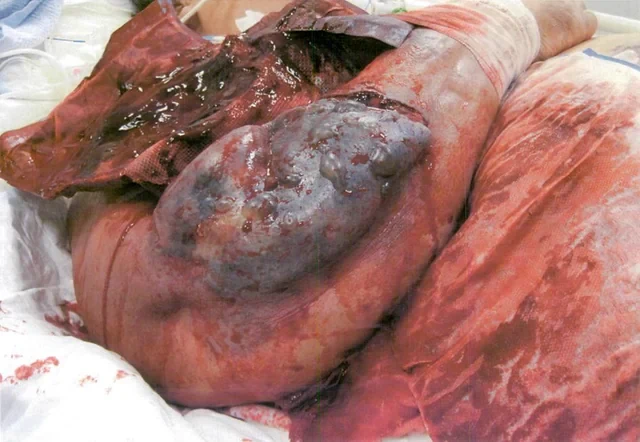
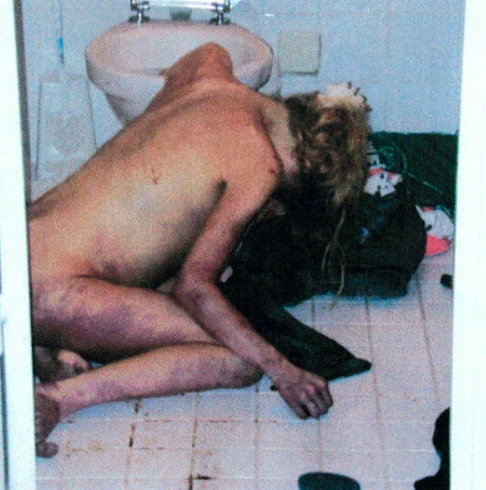
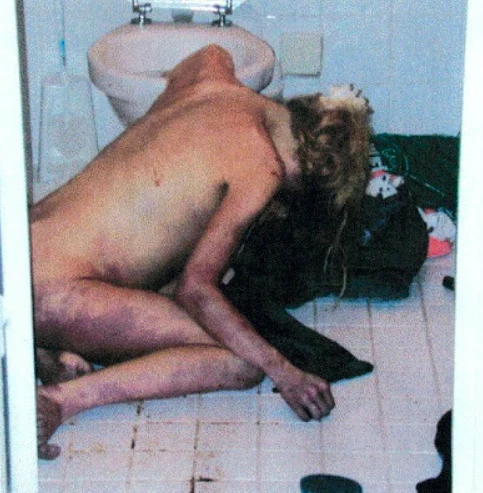
Death due to neurogenic shock following gastric rupture in an anorexia nervosa patient.
"Take notice of her position, the discoloring of her limbs and her stomach. She was 19 and had anorexia and bulimia for 5 years. Died at 5' 1" (155cm) and 94 lbs (43kg) after her stomach ripped after eating 5.6 liters (pic of stomach contents) of food.

Case notes:
She was in full rigor mortis - which is present from 12-72 hours. The bruises set the time frame at around 8+ hours. Her eyes had clouded, which happens at progressively from about 2 -4 hours on. If you look really closely at her stomach, you can see a greenish tint, which is a typical sign of her internal organs decaying - called livor mortis. I think this process may have been accelerated as her insides were digested since it normally takes a few days to set in.
The bruises called for the autopsy. Because of her position when her stomach exploded, it spilled all its contents into her body cavity. The blood and food settled around her anus and vagina and caused what looked like "fresh bruises." So to rule out sexual [assault, etc.], they had to autopsy. When they did the autopsy, they found that her stomach had been extended from where your ribs meet each other all the way to her pubic bone, right behind that pad of fat above the genitals (mons pubis). And her stomach had a large rip in it...
She also had some other abnormalities going on. Her heart was small and displayed typical characteristics of a starving heart - destroyed muscles and dead immune cells (lipofuscin bodies). Her brain had swelled, my guess due to the massive increase in blood flow after her stomach ruptured - it had started to squeeze out her skull before she died. She also had evidence of focal pneumonia in her lungs - not really surprising as starvation hurts the immune response to viruses.
Like a typical binger, her stomach was dying before it ripped. What I mean is that every time we binge our stomachs expand, if they expand far enough, the vessels supplying them blood are crushed - cutting off the blood supply to that area, killing the tissue. That area is weakened and the next binge of that caliber becomes more dangerous. Purging just adds fuel to the fire by increasing stomach pressure above and beyond the natural level.
But believe it or not the ruptured stomach didn't kill her. A natural reaction did. When the stomach exploded, her body responded with a typical immune reaction. It dilated her blood vessels, her blood pressure dropped, she blacked out, and her heart slowed down and stopped. They also did a tox screen and found nothing. Potassium levels are obviously of no use as when you die potassium leaks out of your cells.
Another things to note about this. Back in the 1800s, they determined that the stomach should only be able to hold 4 liters of stuff (by filling corpses). To surpass this, we have to adapt our stomach sizes - resulting in gastric dilatation. Ruptures via overfilling the stomach appear along the lesser curvature of the stomach, whereas vomiting induced ruptures normally occur along the greater curvature and fundus (the top of the stomach) - it's unusual that her stomach ripped how it did, right down the front. Apart from the intellectual value of the report it does illustrate an important point - the endpoint of these diseases is very ugly. "There is no glamour or beauty spending your last living moments over a toilet."
The text isn't mine 
Source:
https://www.2medusa.com/2008/09/bulimia-killswarning-graphic-pictures.html
Hope this was interesting or helpful



- 4
- 17
A 26-year-old African American female not known to have ever been pregnant arrived to the emergency department (ED) via ambulance complaining of a one-day history of progressively worsening vaginal bleeding and crampy lower abdominal pain. Prior to her arrival to the ED, the patient stated that she began passing clots, and while sitting down on the toilet, she attempted to pull out a thick vaginal blood clot. Instead, she reportedly grabbed hold of a pair of legs and pulled out a fetus that was missing its head. She dropped the body of the fetus into the toilet and called EMS, who brought her and a decapitated fetus to the hospital (Figure 1).
The last menstrual period was estimated to be at 2 months prior to the date of presentation. The patient reported taking a home pregnancy test about 1 to 2 weeks before her ED visit that was negative. She had a medical history significant for chronic myeloid leukemia, for which she reports taking Tasigna (nilotinib), a tyrosine kinase inhibitor which is FDA pregnancy category D (positive evidence of risk). Her surgical history is significant for ovarian cystectomy and left oophorectomy.
On examination, the patient appeared well and in no distress. Her vitals were stable and physical exam was unremarkable except for mild suprapubic tenderness to palpation. A transvaginal ultrasound was performed, revealing no intrauterine gestation and a markedly thickened endometrium of up to 3.6 cm. Questionable hyperemia of the anterior myometrium and a probable corpus luteal cyst in the right ovary were also noted. A pelvic exam showed a moderate amount of blood in the vaginal vault, along with the fetal head located at the external cervical os. The fetal head was removed using ring forceps, after which the patient was transferred from the ED to the operating room for dilation and curettage and had an uneventful postoperative course.
The pathology report on the fetus reports a 182-gram phenotypic male with the intestinal organs outside of the abdomen cavity through an omphalocele. There was mild ecchymosis, a laceration in the right groin, and the head was disconnected from the body.




Top Poster of the Day:
 TheBillCollector
TheBillCollector
Deaths Today: 0
Current Registered Users: 2,025,568
 BROWSE EFFORTPOSTS
SITE GUIDE
PING GROUPS
BROWSE EFFORTPOSTS
SITE GUIDE
PING GROUPS
Medical

Aspiring medical student? Or maybe just have an interest in human anatomy? Here you will find everything from autopsies to surgeries to photos from medical journals. If it happened in the operating room or the morgue, it probably belongs here.
 Slavshit
Slavshit

 Sandshit
Sandshit
